

Introduction
Gray-zone lymphoma (GZL) is a rare lymphoid neoplasm initially described in 2005. The world health organization first recognized it as a separate entity in 2008. These tumors have intermediate morphologic and phenotypic features between diffuse large B-cell lymphoma and Hodgkin lymphoma. There is no treatment guidelines given the rarity of the disease, and being relatively a new entity. In this first population-based analysis of GZL, we focus on combined modality treatment (CMT; chemotherapy and radiation) versus chemotherapy alone as a primary treatment strategy. We sought to examine the effect of each modality on survival and investigate clinical and socioeconomic predictors of treatment selection and survival using the national cancer database (NCDB).
Methods
We conducted a retrospective cohort analysis using de-identified data accessed from the NCDB. The NCDB provided records of 2176 patients diagnosed with GZL between 2004 and 2016. We excluded patients without histologic or cytologic confirmation of the diagnosis or patient with unrecorded stage information. We also excluded patients who started treatment after 4 months of diagnosis to account for immortal time bias. Treatment was categorized as CMT or chemotherapy alone. Exploratory analysis of the patient groups was performed. Summary statistics are presented as percentages for categorical data and median with interquartile range for quantitative data. Multivariate regression models were used to analyze the predictors of treatment selection and survival. We used propensity score matching methodology for the comparative survival analysis. Survival estimates were performed using the Kaplan-Meier method and survival differences were assessed using the log-rank test.
Results
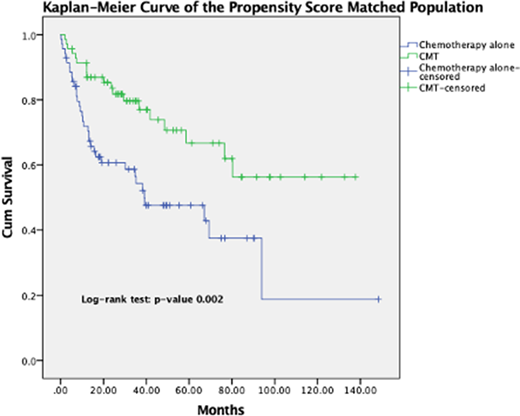
We identified 1047 patients with GZL who were treated with CMT or chemotherapy alone between 2004 and 2016. The median age was 63 (IQR 47-74), there were 56.7% Males. The majority of the patients were non-Hispanic whites (80.7%), had insurance (96.1%), had comorbidity score of 0 (75.4%), belonged to a metropolitan areas (83.4%), and were treated at a comprehensive community cancer centers or academic programs (65.5% combined). Only 164 patients (15.7%) received CMT, while 883 (84.3%) received chemotherapy alone. Treatment selection was affected by clinical factors (age and advanced stage) but not socioeconomic factors. Median follow up for the 811 patients with available survival data was 28.8 months (IQR 12.36-50.25). The use of CMT and higher median income were associated with better survival, while increased age, higher comorbidity score, and presence of B symptoms were associated with worse survival. Median overall survival was significantly higher in CMT group compared with chemotherapy alone group (HR 0.541, 95% CI 0.351-0.833, p-value 0.005).
Discussion
Number of patients with GZL increased gradually over the years, which reflects increased insight and recognition of this disease entity. The use of CMT is continuously increasing over the years. Receiving CMT had a survival advantage over chemotherapy alone. In contrary to a multicenter retrospective analysis by Evans et al where advanced stage was the only important predictor of survival in GZL, our analysis showed other clinical and socioeconomic factors that affected outcomes. Radiation is associated with increased cost, it requires complex planning, and creates significant psychosocial burden, in addition to toxicity which could have contributed to its less use with older patients. A previous retrospective report showed no effect on survival with use of consolidative radiation in 37 patients. Larger sample size in our cohort could have contributed to a different outcome. Our study is limited by its retrospective nature and lack of certain pertinent variables, such as details of chemotherapy regimens. Being a relatively new entity limited median follow up to 2.4 years. Longer follow up and larger prospective studies are needed to evaluate the role of consolidative radiation in GZL and its toxicity. Our study adds to the sparse literature about GZL and identifies clinical and socioeconomic factors that can affect treatment selection and outcome that should be taken in consideration in future research.
Fazal:Jazz Pharma: Consultancy, Speakers Bureau; Amgen: Consultancy, Speakers Bureau; Jansen: Speakers Bureau; Stemline: Consultancy, Speakers Bureau; BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Gilead/Kite: Consultancy, Speakers Bureau; Agios: Consultancy, Speakers Bureau; Incyte Corporation: Consultancy, Honoraria, Speakers Bureau; Karyopham: Speakers Bureau; Celgene: Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Glaxosmith Kline: Consultancy, Speakers Bureau; Takeda: Consultancy, Speakers Bureau. Kahn:AstraZeneca: Honoraria; Celgene: Honoraria; Seattle Genetics: Honoraria; Genetech: Honoraria; Abbvie: Honoraria; Beigene: Honoraria; Takeda: Honoraria; Karyopharm: Honoraria.

